医学科普
发表者:许树才 人已读
Meniscus Cysts: Arthroscopic Debridement, Open Excision or Repair the Defect?
半月板囊肿的治疗:清理,开放切除还是修复?
广东省中医院二沙岛分院骨科 许树柴 主任医师
History历史
Nicaise in 1883 and Ebner in 1904 reported meniscal cysts and considered them to be a hernia of the synovial membrane.
Etiology: 病因
A. Meniscal degeneration (primary or traumatic) usually the primary lesion 半月板退变常常是原发病变。a. Degenerative etiology: results from a degenerative breakdown of the meniscal collagen 半月板胶原的退变。
b. Trauma etiology(创伤): direct compression injury of the peripheral meniscus (Reagan 1989) (Wroblewski 1971 found a trauma in half of 500 cases)
c. Myxoid degeneration of meniscus collagen leads to intrameniscal cyst (半月板胶原退变导致的半月板内囊肿)
d. The cyst progresses peripherally and then outside the meniscus.
e. Synovial fluid collection results from a one‐way valve effect of the tear in usually a horizontal tear. (Barrie 1979 : horizontal cleavage tears in 100% of 112 cysts) (Smillie 1962: 86% of 448 lateral cysts had meniscal damage)
B. Post meniscal repair using suture or repair devices 后侧半月板修复使用缝合或修复工具a. (Yoo 2008) (Nagura 2004) (sutures or meniscal repair devices)
b. Cyst formation may depend on repair device
c. Suture (Kimura 1993) hypothesized that the cyst is caused by cystic degeneration of the meniscus with active fluid secretion after synovial cell invasion along the suture holes. (Nagura 2004) nylon suture repair.
d. All‐inside T‐Fix repair (Lombardo 1999) cyst associated with an all‐inside T‐Fix repair using multiple devices.
e. Meniscal arrow (Tingstad 2001) 4 of 28 arrow repairs resulted in cysts, cystic hematoma formation described (Hechtman 1999)
C. Other theories: latent synovial rest and chronic infection
Incidence of Cysts 囊肿发生率 Orthopedic Literature: Lateral meniscal cysts more frequent than medial meniscus cysts Incidence of lateral meniscal cysts in the population reported between 1.2% ‐19.5%
Seger (1986) reported the ratios between lateral and medial cysts to be 10 to 1 (外侧与内侧半月板囊肿相比是10:1,外侧常见)
Maffuli (1991) found a 5 to 1 ratio in 8100 arthroscopies (5:1)
Hulet (2004) reported only one medial cyst compared to 105 lateral cysts. (100:1 ?)
Mills (1993): (largest reported series of medial cysts) 20 medial cysts out of 7345 knee arthroscopies (0.27%). 15 cysts associated with posterior horn meniscus tears while 3 cysts had no associated meniscus tear. >50% of these tears were horizontal cleavage tears
Lateral cyst incidence外侧半月板囊肿发生率: 1.5% of a series of 8100 knee arthroscopies (Hulet 2004)
1.2% in a series of 1160 arthroscopies (Passler 1993)
Meniscal tear types associated with lateral meniscal cysts (Hulet 2004) 撕裂的类型。
Horizontal tear水平 28.5%
Horizontal w/ radial split 水平/根部28.5%
Radial split根部 29%
Complex tear混合 10%
Vertical tear垂直 4%
Location of lateral tear 外侧撕裂
Anterior horn 前角22%
Middle horn 体部71%
Posterior horn 后角1%
Combined复合 6%
Radiology Literature: (different perspective!) 放射影像学文献Tasker (1995) reported 50 MRI proven meniscal cysts (28 medial and 22 lateral).
Most common sites were the posterior medial 1/3 & lateral mid‐third.
Only 15 of 50 cysts were suspected clinically (5 medial and 10 lateral).
Campbell (2001) 2572 knee MRIs: 109 meniscal cysts (66% medial and 34% lateral)
Cysts ranged in widest diameter from a low of 0.3mm (clinically insignificant?)
De Smet (2011) 7771 knee MRIs: 138 meniscal cysts (64% medial and 36% lateral)
Medial knee cyst with complex tear medial meniscus after kickboxing injury (Campbell AJR 2001)
Some meniscal cysts may not be true cysts: 某些半月板囊肿可能不是真的囊肿Iatrogenic (after meniscal repair implant) (Yoo 2008)
If not, it may be better treated conservatively after the underlying disease is corrected
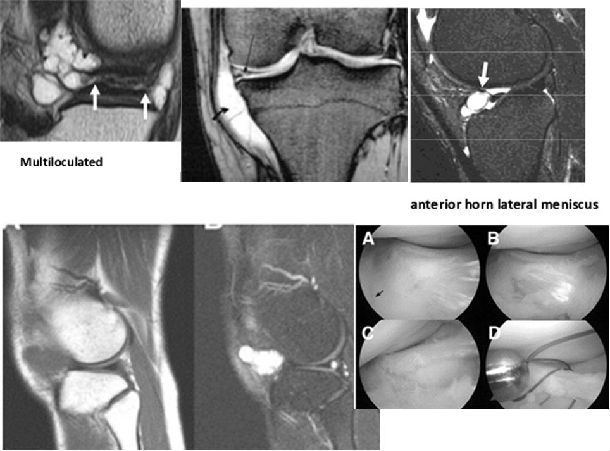
Types of meniscal cysts()半月板囊肿的类型
? Single versus multi‐loculated (单一或多发,多个)
? Anterior versus mid lateral or posterior medial
? Endothelial lining with synovial like fluid versus poorly defined fibrotic stroma
? Ganglion cyst? ganglion cysts contain a jelly like viscous fluid
Symptoms 症状学Chronic, well tolerated pain progressing over time
Localized joint line swelling (usually laterally) which may become noticeably more
prominent in external rotation, and completely disappear with internal rotation (Pinar 2009)
Pisani's Sign: disappearance of the lateral cyst swelling with knee flexion
Rarely, common peroneal nerve palsy (Jowett 2008)
Imaging 影像学Radiographs: may reveal a soft tissue mass shadow 影像学可能有软组织阴影。
Ultrasonography: operator dependent (超声与操作者经验有关)
Magnetic resonance imaging: the definitive test (MRI检查准确)
Treatment: deal with the meniscus and then deal with the cyst (pathology dependant) :治疗需要考虑半月板及囊肿本身,两者兼顾。
Most series report tears consistently present with a lateral meniscus cyst
1. Arthroscopy, partial meniscectomy to remove the flap valve effect (usually inferior shelf of a horizontal tear) sufficient to allow intra‐articular cyst decompression and drainage (Parisien 1990, Ryu 1993, Mills 1993, Glasgow 1993)
a. 85% good to excellent results
b. Remove all yellowish degenerative tissue!
2. Arthroscopic partial meniscectomy and open cyst removal
a. Only if the cyst does not decompress (small radial tears)
3. For peripheral, vertical meniscal tears: consider meniscal repair is patient and meniscus is suitable
a. Should have a high expectation of meniscal healing
4. Arthroscopic internal marsupialization of meniscal cysts with or without meniscectomy (Howe 2007).
a. A 5 mm channel is arthroscopically created in the capsule adjacent to the cyst to decompress the cyst into the joint and equalize pressures between the cyst and joint. 8 MRI confirmed atraumatic medial or lateral meniscal cysts were reported. (Howe 2007)
b. Yoo (2008) Arthroscopic partial cystectomy of only the intra‐articular portion of the cyst: successfully resolved the issue without removing the extra‐articular part of the cyst.
5. Anterior lateral cyst: Outside‐in anterior horn meniscal suture repair and needle aspiration of cyst (Lu 2006) or decompression of a large cyst (Ahn 2006)
a. The meniscal tear is freshened arthroscopically (without destroying the communication track or the cyst) and repaired with an outside‐in #3‐0 nylon suture passed into the joint with a needle and retrieved through a separate portal. Sutures are spaced 8 to 10 mm apart. The cyst is then decompressed by aspiration.
6. No meniscal tear: (arthroscopic confirmation) open cyst excision recommended. (Pedowitz 1996)
7. Solitary meniscal cyst invading the infrapatellar fat pad with no meniscal tear: treated with needle aspiration and steroid injection but not meniscectomy (Liu KSSTA 2007)
Pearls 技巧与经验1. Carefully screen the MRI preop to assess the presence and location of the cyst and associated meniscal tear (preop planning and counseling of patient).
2. Carefully probe the inferior and superior aspects of the meniscus for any small tear which could open into a large intrameniscal cleavage plane.
3. Remove any yellow pathologic meniscal tissue (go anterior and posterior)
4. Stop when macroscopically normal meniscal tissue is exposed.
5. Posterior laterally, be conservative in resection and try to preserve a meniscal bridge at the popliteal hiatus.
6. Recurrence rates can approach 10% (Maffulli; Hulet). Good news: reoperation does not compromise final outcome.
Conclusions 结果 An analysis of the literature must consider how the diagnosis of meniscal cysts was made (cadaver dissection, arthrotomy, arthroscopy, or MRI), the treatment used (arthrotomy or arthroscopy), and who is making the call (orthopedic surgeon or
radiologist).
Predominant meniscus tear type: horizontal cleavage
Most common location of lateral cysts: middle third of the meniscus
Most common location of medial cysts: posterior third of the meniscus
Anterior meniscal cysts may be a different type of problem.
Small cysts were only clinically predicted on the lateral side suggesting that medial cysts are more common than lateral and more difficult detect clinically.
The rationale for limited open cyst excision is meniscal preservation. The general principles relating to meniscal repair should apply including the nature of the meniscal tissue (degenerative?), vascular supply, patient age and knee alignment and stability.
The surgeon should consider the appropriateness of repairing a meniscus with demonstrated myxoid degeneration.
Treatment Algorithm (Pedowitz 1996) 治疗流程 Suspect Meniscal Cyst ? MRI ? No Cyst (do nothing) 半月板囊肿筛查?
Meniscal cyst present ? arthroscopy and evaluate for meniscal tear 半月板囊肿存在,做关节镜检查及半月板撕裂评估
Meniscal tear present ? Arthroscopic partial meniscectomy and cyst decompression 如果半月板撕裂存在,做半月板部分切除成型及囊肿减压。
Meniscal tear absent ? open cyst excision and meniscal repair 然后半月板撕裂不存在,做开放囊肿切除及半月板修复。
References: 参考文献
1.Campbell SE, Sanders TG, Morrison WB. MR imaging of meniscal cysts: incidence,
location, and clinical significance. AJR Am J Roentgenol. 2001;177(2):409‐413.
2.De Smet AA, Graf BK, del Rio AM. Association of parameniscal cysts with underlying
meniscal tears as identified on MRI and arthroscopy. AJR Am J Roentgenol. 2011;
196(2):W180‐6.
本文是许树才版权所有,未经授权请勿转载。 本文仅供健康科普使用,不能做为诊断、治疗的依据,请谨慎参阅
发表于:2015-01-03










